TPHA Test: Principle, Procedure, Results, and Interpretation for Syphilis Confirmation
TPHA (Treponema pallidum Haemagglutination Assay) is the standard treponemal confirmatory test for syphilis. Learn its passive haemagglutination principle, microtiter procedure, reactive vs non-reactive results, false positives, and when to use TPHA vs FTA-ABS.
A 28-year-old man presents to a sexual health clinic after a routine screening reveals a reactive RPR at a titer of 1:8. He has no symptoms — no rash, no genital ulcer, nothing clinically apparent. He is alarmed. His clinician explains that the RPR is a screening test that can be falsely positive in several conditions including recent viral infections, autoimmune diseases, and certain chronic illnesses.
Before treatment is considered, a confirmatory treponemal test is needed. This is where TPHA comes in. Unlike the RPR — which measures antibodies to cardiolipin, a lipid found in many tissues — the TPHA specifically detects antibodies against Treponema pallidum, the causative organism of syphilis. If the TPHA is reactive, syphilis infection (past or present) is confirmed. If non-reactive, the RPR result is most likely a biological false positive.
The TPHA is the most widely used treponemal confirmatory test globally, preferred over the FTA-ABS in routine clinical settings because it requires no fluorescence microscope, produces objective readable results, and is available from multiple commercial manufacturers at accessible cost.
Treponema pallidum Hemagglutination Assay (TPHA) is a treponemal test for the serologic diagnosis of syphilis, a sexually transmitted infection caused by spirochetes, Treponema pallidum. Based on the principle of passive haemagglutination, this test detects anti-treponemal antibodies (IgG and IgM antibodies) in serum or CSF. TPHA has been used as a confirmatory test for the diagnosis of Treponema pallidum infection since the mid-1960s. TPHA is a good primary screening test for syphilis at all stages beyond the early primary stage.
TPHA in the Syphilis Serology Framework
Understanding where TPHA fits in syphilis diagnosis requires knowing the full test landscape:
| Test | Type | Detects | Reactive in past treated infection? | Main use |
|---|---|---|---|---|
| RPR / VDRL | Non-treponemal | Anti-cardiolipin (reagin) antibodies | No (usually reverts after treatment) | Screening + treatment monitoring |
| TPHA / TPPA | Treponemal | Anti-T. pallidum antibodies (IgG + IgM) | Yes — for life | Confirmatory test; most widely used |
| FTA-ABS | Treponemal | Anti-T. pallidum antibodies (IgG + IgM) | Yes — for life | Confirmatory; more sensitive in early primary |
TPHA's specific role:
- Confirms a reactive non-treponemal result (RPR or VDRL)
- Distinguishes true syphilis from biological false-positive non-treponemal tests
- Used in epidemiological surveys for syphilis prevalence
- Cannot be used to monitor treatment response (remains reactive for life)
- Less sensitive than FTA-ABS in very early primary syphilis (window period)
The important limitation to state explicitly: TPHA will remain reactive for life in a person who was successfully treated for syphilis years ago. A reactive TPHA in someone with a low or non-reactive RPR most likely represents past treated infection, not active disease requiring treatment.
Principle
TPHA test is a passive hemagglutination assay based on hemagglutination of erythrocytes sensitized with T. pallidum antigen by antibodies found in the patient’s serum or plasma. It is used for both qualitative and semi-quantitative detection of anti-treponemal antibodies.
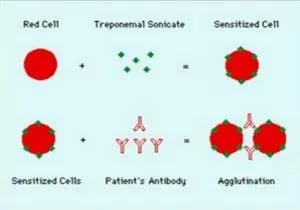 Figure: TPHA Test Principle
Figure: TPHA Test Principle
The test sample is diluted in absorbing diluent to remove possible cross-reacting heterophile antibody and to remove, block, or absorb potentially cross-reacting, nonpathogenic treponemal antibodies. Sera containing antibodies to T. pallidum react with erythrocytes (chicken or avian) sensitized with sonicated T. pallidum, Nichols strain (the antigen), to form a smooth mat of agglutinated cells in the microtiter tray well. If antibodies are not present the cells settle to the bottom of the tray well, forming a compact button of unagglutinated cells.
Sensitivity of TPHA by Stage of Syphilis
| Stage | TPHA sensitivity | Clinical note |
|---|---|---|
| Primary (very early, <3 weeks) | ~65–76% | Window period — TPHA may be negative in early primary syphilis; FTA-ABS becomes positive earlier |
| Primary (established chancre) | ~76–84% | Use FTA-ABS if TPHA is negative but primary syphilis is clinically suspected |
| Secondary | ~100% | All treponemal tests reactive |
| Latent (early and late) | ~97–99% | Highly sensitive; reliable for latent disease screening |
| Late/tertiary | ~99% | Very sensitive at this stage even when RPR may be low |
The early primary gap: TPHA is less sensitive than FTA-ABS in the first 3–4 weeks of primary infection. In a patient with a suspicious genital ulcer and a non-reactive TPHA, FTA-ABS should be requested to avoid missing early primary syphilis. Darkfield microscopy of the chancre (where available) is the most sensitive test in this window.
Uses of TPHA
- Confirmatory testing after reactive non-treponemal screen: The primary use — confirming that a reactive RPR or VDRL represents true treponemal infection rather than a biological false positive.
- Epidemiological syphilis surveillance: Population-level syphilis prevalence surveys use TPHA because it is objective, reproducible, and can be performed on stored sera without the reader-dependent variation of fluorescence microscopy (FTA-ABS).
- Blood bank screening: Some blood transfusion services use TPHA alongside or instead of non-treponemal tests for donor screening.
- Antenatal screening panel: In settings with higher syphilis prevalence, a combined screen (RPR + TPHA) improves both sensitivity and specificity compared to single-test screening.
- Semi-quantitative titer for baseline: TPHA can be performed quantitatively (serial doubling dilutions), providing a baseline treponemal antibody titer, though this is less clinically useful than RPR titers for monitoring because treponemal titers do not fall predictably with treatment.
Reagents (supplied by manufacturers)
- Test cell suspensions: Preserved RBCs treated with tannic acid and coated with T. pallidum antigen.
- Control cell suspension: Preserved RBCs (without immobilized T. pallidum antigen)
- Buffer: Phosphate buffered saline solution containing adsorbers (used to remove possible cross-reacting heterophile antibodies).
- Positive Control serum: Human serum containing antibodies against T. pallidum. Ready for use. This will give an equivalent titer of 1/640 to 1/2560 with the quantitative test.
- Negative Control serum: Human serum free of antibodies against T. pallidum
Procedure
Before performing the test procedure, bring the sample, diluent, control, and test cells at room temperature (25 – 30ºC). For each qualitative test, a test card with three wells is needed.
A:Dilution of serum sample
- Add 10μL of patient’s serum in the first well (say well A).
- Add 190 μL of diluent (provided by the manufacturer).
- Mix the content well using a micropipette; we will use this diluted serum later.
B: Testing of serum sample for the presence of specific antibodies
- Add 75μL of “control cells” to well B and 75 μL of “test cells” to well C.
- Add 25μL of diluted serum on each B and C well.
- Shake the plate gently to mix the contents thoroughly.
- Cover the plate and protect to direct sunlight, heat and any source of vibration.
- Incubate 45-60 minutes at room temperature.
- Read the test results and interpret.
Positive control and negative control should be run along with the test serum (see quality control section below).
Results and Interpretation
If the controls (positive control and negative control) do not give the expected result, all assays performed in that batch are invalid and must be tested again.
| Results | Test Cells | Control Cells |
|---|---|---|
| Strongly Reactive | Full cell pattern covering the bottom of the well. | No agglutination tight button |
| Weakly Reactive | Cell pattern covers approx. 1/3 of well bottom | No agglutination tight button |
| Indeterminate (Equivocal) | Cell pattern shows a distinctly open centre | No agglutination tight button |
| Nonreactive | Cells settled to a compact bottom, typically with a small clear center. | No agglutination tight button |
- Reactive (R): Reactive results may indicate an active, past, or successfully treated infection. A diagnosis should be made with a careful history of the patient and a physical examination as well as pertinent laboratory results.
- Indeterminate: indeterminate results are confirmed with the MHATP and FTA-ABS test tests.
- False Positive results: Although TPHA test is highly specific, false-positive results have been known to occur in patients suffering from leprosy, infectious mononucleosis, and connective tissue disorders. For confirmation, FTA-ABS test should be used.
Distinguishing true positive from false positive TPHA: A reactive TPHA in the context of clinical signs or symptoms of syphilis, or alongside a reactive RPR, strongly suggests true infection. A reactive TPHA with a non-reactive RPR in an asymptomatic patient most likely represents either: (1) past successfully treated syphilis (the most common scenario in practice), or (2) a rare false-positive TPHA in one of the conditions listed above. Clinical history is essential: document any previous syphilis treatment, review old records, and consider whether the patient has lived in or travelled to areas where non-venereal treponematoses (yaws, bejel, pinta) are endemic — these will also give reactive TPHA results indistinguishable from venereal syphilis.
Quality Control
Positive and negative control are included in the test kit for the quality control. Control should be recommended in the following cases:
- At least once a run
- At least once within 24 hours
- When changing vial of reagent.
If the control is not showing expected results; the test is invalid (whatever be the test results).
Similar Tests
- Treponema pallidum Particle Assay (TP-PA) is another treponemal test. It uses gelatin particles as carrier molecules. Some studies have reported that TPPA has higher sensitivity than the TPHA in detecting cases of primary stage syphilis.
- Microhemagglutination Assay for Treponema pallidum (MHA-TP): It is another confirmatory test to detect treponemal antibodies. This test is used much less commonly now.
- Treponema pallidum immobilization (TPI) test This test measures the presence of antibodies against Treponema pallidum in the patient’s serum.T. pallidum (Nichols strain) grown in rabbit testes is used as the antigen. If the patient’s serum contains antibodies against treponema, antibody and complement immobilizes the living treponemes. The test results are read by dark-field microscopy. Failure to immobilize the treponema strain suggests the absence of antibody in the patient’s serum, thus not infected with syphilis. TPI test is technically difficult, expensive, time-consuming so rarely performed nowadays.
How to Remember
TPHA = T. pallidum-coated red cells that clump when antibody is present.
The test is conceptually simple: red blood cells are coated with T. pallidum antigen. If the patient has anti-treponemal antibodies, those antibodies bridge adjacent red cells, causing them to agglutinate into a mat covering the well floor. No antibody = cells settle into a tight button at the centre of the well. The pattern is read visually — no microscope needed, which is the key practical advantage over FTA-ABS.
The passive haemagglutination principle: Unlike direct haemagglutination (where the organism itself agglutinates red cells), TPHA is passive — the red cells are just carriers of the treponemal antigen. The antibody bridges the antigen-coated cells together. The word "passive" is the clue: the cells are passive carriers, not the active participants in the reaction.
The two confirmatory test decision:
- TPHA first: standard routine choice; no fluorescence microscope; objective result
- FTA-ABS if TPHA is negative but primary syphilis is still suspected: more sensitive in the early primary window (3–4 weeks post-infection)
Reading the well:
- Mat pattern (cells cover the whole well floor) = reactive — think "spreading out = positive"
- Button (cells in tight central cluster) = non-reactive — think "clumping together = negative"
This is counterintuitive — clumping sounds like a positive result, but in TPHA it is the non-reactive pattern. Remember: the mat (spread) is positive; the button (tight) is negative.
References
- Kashyap, B., Goyal, N., Gupta, N., Singh, N. P., & Kumar, V. (2018). Evaluation of Treponema pallidum Hemagglutination Assay among Varying Titers of the Venereal Disease Research Laboratory Test. Indian journal of dermatology, 63(6), 479–483. https://doi.org/10.4103/ijd.IJD_595_17
- Gupta, K., Bhardwaj, A., Dash, S., & Kaur, I. R. (2018). Role of Treponema pallidum hemagglutination assay for diagnosis of syphilis in low titers of VDRL-reactive sera: A prospective study from a large tertiary care center of East Delhi. Journal of family medicine and primary care, 7(6), 1594–1595. https://doi.org/10.4103/jfmpc.jfmpc_258_18
- Larsen S.A., Steiner B.M., Rudolph A.H. (1995). Laboratory diagnosis and interpretation of tests for syphilis. Clinical Microbiology Reviews, 8(1), 1–21.
- Centers for Disease Control and Prevention. (2021). Sexually Transmitted Infections Treatment Guidelines, 2021: Syphilis. MMWR, 70(4).
- Tille, P. M. (2017). Bailey and Scott's Diagnostic Microbiology (14th ed.). Elsevier.
Frequently Asked Questions
How is the TPHA result read from the microtiter well and what distinguishes a mat pattern from a button pattern?
Can the TPHA test distinguish between different treponemal infections, such as syphilis versus yaws?
What does an isolated reactive TPHA with non-reactive RPR mean, and how should it be managed?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.