Ziehl-Neelsen Staining: Principle, Procedure, Grading, and Interpretation
Ziehl-Neelsen (ZN) staining detects acid-fast bacilli in sputum and other specimens. Learn the hot and cold methods, AFB grading scale, smear reporting, troubleshooting, and when to use fluorochrome staining instead.
A 35-year-old man presents with three weeks of productive cough, night sweats, and weight loss. A chest X-ray shows an upper lobe cavity. The clinician requests a sputum smear for AFB.
In many parts of the world — including Nepal, India, and most of sub-Saharan Africa — the Ziehl-Neelsen smear result is the first and sometimes only microbiological evidence available before treatment decisions are made. Culture may take 6–8 weeks on Löwenstein-Jensen medium. Molecular tests (GeneXpert) may not be accessible. The ZN smear, available within hours, guides whether to start anti-TB therapy in a patient who cannot wait.
Learning ZN staining is not an academic exercise. In high-burden settings, it is a clinical skill with direct impact on patient outcomes.
Ziehl-Neelsen (ZN) acid-fast staining technique is used to stain Mycobacterium species, including M. tuberculosis, M. ulcerans, M. leprae, and nontuberculous mycobacteria (NTM). Detection of acid-fast bacilli (AFB) in stained and acid-washed smears examined microscopically may provide the initial bacteriologic evidence of the presence of mycobacteria in a clinical specimen. Smear microscopy is the quickest and easiest procedure that can be performed.
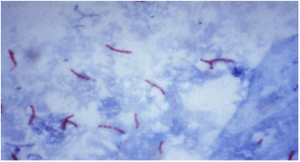 Figure: Acid-fast bacillus (AFB) in Z.N smear
Figure: Acid-fast bacillus (AFB) in Z.N smear
Mycobacteria’s cell wall contains high lipid concentrations, making them waxy, hydrophobic, and impermeable to routine stains such as the Gram Stain. They are also resistant to acid and alcohol and are described as acid-fast bacilli (AFB)or acid alcohol fast bacilli (AAFB).
There are two procedures commonly used for acid-fast staining:
- Carbolfuchsin methods which include the Ziehl-Neelsen and Kinyoun methods (light/bright field microscope)
- Fluorochrome procedure using auramine-O or auramine-rhodamine dyes(fluorescent microscope).
Principle of Ziehl-Neelsen Method of Acid-Fast Staining
Mycobacteria, which do not stain well by Gram stain, stains well with carbol fuchsin combined with phenol.
- In the ‘hot’ ZN technique, the phenol-carbol fuchsin stain is heated to enable the dye to penetrate the waxy mycobacterial cell wall.
- In the ‘cold’ technique known as Kinyoun Method, stains are not heated but the penetration is achieved by increasing the concentration of basic fuchsin and phenol and incorporating a ‘wetting agent’ chemical.
The stain binds to the mycolic acid in the mycobacterial cell wall. After staining, an acid decolorizing solution is applied. This removes the red dye from the background cells, tissue fibres, and any organisms in the smear except mycobacteria which retain (hold fast to) the dye and are therefore referred to as acid-fast bacilli (AFB).
Following decolorization, the sputum smear is counterstained with malachite green, or methylene blue which stains the background material, providing a contrast color against which the red AFB can be seen.
Among the Mycobacterium species, M. tuberculosis and M. ulcerans are strongly acid-fast. When staining specimens for these species, a 3% v/v acid alcohol is used to decolorize the smear, whereas M. leprae is only weakly acid-fast. 0.5-1% v/v decolorizing solution is therefore used for M. leprae smears and also different staining and decolorizing time.
Note: 0.5% Acid alcohol or 5% Sulphuric acid is used for Atypical AFB because they (eg. Mycobacterium leprae, Nocardia asteroides) are much less acid and alcohol fast than Mycobacterium tuberculosis bacilli.
 Figure: Fig. Heat Fixation of smear (Upper: using an electric heater, lower: using burner)
Figure: Fig. Heat Fixation of smear (Upper: using an electric heater, lower: using burner)
ZN vs Fluorochrome Staining: Which to Choose?
Two methods are used for acid-fast staining in clinical laboratories. The choice depends on workload, available equipment, and the clinical urgency.
| Feature | Ziehl-Neelsen (Carbolfuchsin) | Auramine-Rhodamine (Fluorochrome) |
|---|---|---|
| Microscope required | Ordinary bright-field microscope | Fluorescence microscope (UV light source) |
| AFB appearance | Red rods on blue/green background | Bright yellow-orange rods on dark background |
| Scanning magnification | 100x oil immersion (entire examination) | 25x or 40x dry objective (scan); 100x to confirm |
| Time to screen one slide | 15–20 minutes | 3–5 minutes |
| Sensitivity vs ZN | Reference standard | Higher — detects paucibacillary specimens better |
| Specificity | High | Slightly lower — artefacts can fluoresce |
| Cost | Low reagent cost | Higher (fluorescence microscope) |
| WHO recommendation | Acceptable | Preferred where fluorescence microscope available |
| Confirmation of positive | Not required | Confirm with ZN if uncertain |
Key point: Auramine-rhodamine is more sensitive than ZN for direct smear examination because slides can be scanned at lower magnification, covering more area per unit time and detecting fewer bacilli. A specimen with 100 AFB/mL may be missed on ZN but detected on auramine-rhodamine. WHO recommends fluorochrome staining as the preferred method where fluorescence microscopy is available.
A positive auramine-rhodamine result that is clinically unexpected should be confirmed by ZN staining of the same slide — fluorescence artefacts (dust, fibres) can occasionally give false-positive results.
For the full procedure for auramine-rhodamine staining, see: Auramine-Rhodamine Fluorochrome Staining
Sample Collection & Preparation
Due to overnight accumulation of secretions, first morning specimens are more likely to yield better recovery of AFB.
- Direct Smear: Smear prepared directly from a patient specimen prior to processing.
- Indirect Smear: Smear prepared from a processed specimen after centrifugation (is used to concentrate the material)
Assessing Sputum Quality Before Staining
The sensitivity of ZN smear microscopy depends critically on specimen quality. A saliva sample labelled as sputum will give a false-negative result regardless of how perfectly the staining is performed.
Before preparing a smear, assess the specimen macroscopically:
| Specimen Appearance | Assessment | Action |
|---|---|---|
| Mucopurulent — thick, opaque, yellow/green | Acceptable | Proceed with smear preparation |
| Blood-stained — rust or red tinged | Acceptable | Note blood-staining; proceed |
| Mucoid — slightly opaque, stringy | Acceptable | Select the most opaque portion |
| Salivary — thin, watery, frothy | Unacceptable | Request repeat specimen |
| Very small volume (<1 mL) | Borderline | Process but note volume; request repeat |
For smear preparation: Always select the most purulent, caseous, or blood-stained portion of the specimen — this is where AFB are most concentrated. Spreading too thin misses AFB; spreading too thick prevents proper decolourisation.
Smear size: Approximately 2 × 3 cm. When dry, the smear should be just readable through (you should be able to read newsprint through it). Too opaque = too thick.
Reagents required
- Carbol fuchsin stain (filtered)
- Acid alcohol 3% v/v (or 20% sulfuric acid)
- Malachite green 5 g/l (0.5% w/v) or Methylene blue, 5g/l
Ziehl-Neelsen Staining Procedure
Procedural note
- Acid alcohol is flammable; therefore, use it with care.
- Take great care while heating carbol fuchsin (as the staining rack may contain volatile chemicals) to reduce the fire risk.
- Slides must not touch each other when placed on a staining rack to prevent the transfer of materialfrom one slide to another.
Results of Acid Fast Staining
- AFB: red, straight, or slightly curved rods, occurring singly or in small groups, may appear beaded.
- Cells: green
- Background material: green
| Reagent | Acid Fast | Non-Acid Fast |
|---|---|---|
| Carbol fuchsin with heat | Red (hot pink) | Red (hot pink) |
| Acid alcohol | Red | Colorless |
| Methylene blue/malachite green | Red | Blue/green |
Troubleshooting ZN Staining
| Problem | Likely Cause | Action |
|---|---|---|
| No red bacilli seen but TB strongly suspected | Paucibacillary specimen; inadequate decolourisation time | Request early morning specimen × 3 consecutive days; use sodium hypochlorite concentration technique; consider fluorochrome staining |
| Background too dark (heavy blue/green staining) | Counterstain applied too long; smear too thick | Reduce counterstain time to 1 minute; prepare thinner smear |
| AFB appear faded/pale pink rather than red | Carbol fuchsin too dilute or expired; heating insufficient | Replace carbol fuchsin; ensure steam rises during heating without boiling |
| Red artefacts appearing (non-AFB structures) | Food particles, vegetable fibres in sputum; scratch on slide | Select purulent portion of specimen; use scratch-free slides; examine morphology carefully (AFB are straight or slightly curved rods, not irregular) |
| Smear washing off during staining | Inadequate heat fixation | Ensure complete air-drying before fixation; increase heat fixation passes; consider methanol fixation |
| Carbol fuchsin does not steam during hot technique | Flame too low; slide holder interference | Adjust flame; ensure slide is not resting on an insulating surface |
The 1-9 AFB/100 fields dilemma: When scanty AFB are found (1–9 per 100 fields), the grading guidelines recommend reporting the exact number and requesting a repeat specimen. This is because saprophytic NTM from tap water, glass slide scratches, or contaminated staining reagents can occasionally produce a false-positive result at very low counts. Always correlate with clinical findings — a patient with a classic TB presentation and 2 AFB/100 fields is a different situation from an asymptomatic person with 1 AFB/100 fields found incidentally.
Grading of sputum smear for *Mycobacterium tuberculosis*
Sputum smear is graded as scanty, 1+, 2+, and 3+.
| Observation | Grading |
|---|---|
| No AFB seen while observing more than 300 fields | No AFB seen |
| 1-9 AFB/100 fields | Report the exact number |
| 10-99 AFB/ 100 fields | Report as 1+ |
| 1-10 AFB/field at least in 50 fields | Report as 2 + |
| More than 10 AFB/field at least in 20 fields | Report as 3+ |
- When no AFB is seen after examining 300 fields, report the smear as ‘No AFB seen’.
- When very few AFB are seen i.e. when only 1 or 2 AFB are seen after examining 100 fields, request a further specimen to examine (that AFB might have come from tap water (saprophytic mycobacteria), or it may be scratch of a glass slide or by the use of the same piece of blotting paper while drying.
- When any red bacilli are seen, report the smear as ‘AFB positive’ and give an indication of the number of bacteria present as follows (the greater the number, the more infectious the patient).
Important: The grading scale shown above follows WHO/IUATLD recommendations. Some laboratories use slight variations — always follow your national TB programme guidelines. The key principle across all systems is that higher grades correlate with greater infectiousness and higher organism burden.
Grading is not just administrative — it has clinical implications:
- A 3+ smear-positive patient is highly infectious and requires immediate isolation precautions
- A patient converting from 2+ to negative on treatment can be used to monitor treatment response
- Smear grades should be documented at treatment initiation (month 0) and at months 2, 5, and 6 to track bacteriological response per national TB programme guidelines
Partial acid-fast organisms (Nocardia, Cryptosporidium, Isospora) require modified decolourisation — 0.5% sulphuric acid rather than 3% acid-alcohol — and should not be reported on the standard TB smear report. If these organisms are clinically suspected, a modified ZN preparation should be specifically requested and clearly labelled.
Advantages
- Microscopy of sputum smears is simple and inexpensive, quickly detecting infectious cases of pulmonary TB;
- Sputum specimens from patients with pulmonary TB – especially those with the cavitary disease – often contain sufficiently large numbers of acid-fast bacilli to be readily detected by microscopy.
Limitation of AFB Microscopy
- Does not distinguish between viable and dead organisms
Follow-up specimens from patients on treatment may be smear-positive yet culture negative
- Microscopy for acid-fast bacilli (AFB) cannot distinguish drug-susceptible from drug-resistant strains.
- Limited sensitivity
High bacterial load 5,000-10,000 AFB /mL is required for detection ( In contrast, 10 to 100 bacilli are needed for a positive culture). Smear sensitivity is further reduced in patients with extra-pulmonary TB, HIV-co-infection, and those with disease due to nontuberculous mycobacteria (NTM). Many TB patients have negative AFB smears with a subsequent positive culture. Negative smears do not exclude TB disease.
- Limited specificity
All mycobacteria are acid-fast Does not provide species identification Local prevalence of MTB and NTM determine the predictive values of a positive smear for MTB
List of Acid Fast Organisms
- Mycobacterium tuberculosis
- Mycobacterium leprae(weak acid-fast)
- Other Mycobacteria
- Nocardia spp: Partial acid-fast
- Rhodococcus spp: Partial acid-fast
- Legionella micdadei: Partially acid-fast in tissue
- Cyst of Cryptosporidium: Acid-fast
- Cyst of Isospora: Acid-fast
Sodium Hypochlorite Centrifugation Technique to Concentrate AFB
This technique is used to concentrate the AFB present in sputum, as it increases the chances of detecting AFB in sputum smears. Sodium hypochlorite (NaOCl) is recommended for liquefying the sputum, as it kills M. tuberculosis, making handling specimens safe for laboratory technicians.
Procedure
- Transfer 1-2 ml of the sputum’s purulent part (i.e. containing any caseous materials) to a screw cap universal bottle or other containers of 10-20 ml capacity.
- Add an equal volume of concentrated sodium hypochlorite (bleach) solution and mix well.
- Leave at room temperature for 10-15 minutes, shaking at intervals to break down the mucus in the sputum.
- Add about 8 ml of distilled water and mix well.
- Centrifuge at 3000 g for 15 minutes. When centrifugation is not possible, leave NaOCl-treated sputum to sediment overnight.
- Remove and discard supernatant fluid using a glass Pasteur or plastic bulb pipette. Mix the sediment.
- Transfer a drop of well-mixed sediment to a clean scratch-free glass slide and spread the sediment to make a thin preparation and allow air-drying.
- Heat fix the smear, stain it using the Ziehl-Neelsen technique, and examine it microscopically.
How to Remember: ZN Staining
Why mycobacteria are acid-fast — the mycolic acid memory hook: Mycobacteria have a waxy cell wall rich in mycolic acid — long-chain fatty acids that make the wall hydrophobic and impermeable. The carbol fuchsin dye penetrates this waxy wall only with heat (hot ZN) or increased dye concentration (cold/Kinyoun method). Once inside, the dye is held so tightly by the mycolic acid that even acid-alcohol — one of the strongest decolourising agents used in microbiology — cannot remove it. Everything else in the smear decolourises; the AFB holds fast. That is where "acid-fast" comes from.
Reagent sequence — "Can Anyone Make Mycobacteria Colourful?"
- Carbol fuchsin — primary stain (all cells red)
- Acid-alcohol — decolouriser (removes red from everything except AFB)
- Malachite green / Methylene blue — counterstain (background turns green/blue)
Grading memory:
- Scanty = 1–9 per 100 fields (report exact count)
- 1+ = 10–99 per 100 fields
- 2+ = 1–10 per field (50 fields)
- 3+ = >10 per field (20 fields)
The numbers increase with grade — more AFB, more infectious, higher grade number.
Key Exam Facts in One Table
| Feature | Detail |
|---|---|
| Full name | Ziehl-Neelsen acid-fast (carbolfuchsin) staining |
| Principle | Mycolic acid in mycobacterial cell wall retains carbol fuchsin after acid-alcohol decolourisation |
| AFB appearance | Red/pink rods; straight or slightly curved; may appear beaded |
| Background colour | Blue (methylene blue) or green (malachite green) |
| Hot technique | Carbol fuchsin heated until steam rises (3–5 minutes); standard ZN |
| Cold technique (Kinyoun) | No heat; higher concentrations of fuchsin and phenol + wetting agent |
| Decolouriser for MTB | 3% acid-alcohol (strongly acid-fast) |
| Decolouriser for M. leprae / Nocardia | 0.5–1% acid-alcohol or 0.5–5% sulphuric acid (weakly/partially acid-fast) |
| Grading: scanty | 1–9 AFB per 100 fields — report exact count, request repeat |
| Grading: 1+ | 10–99 AFB per 100 fields |
| Grading: 2+ | 1–10 AFB per field in 50 fields |
| Grading: 3+ | >10 AFB per field in 20 fields |
| Fluorochrome alternative | Auramine-rhodamine — higher sensitivity, faster screening, requires fluorescence microscope |
| Organisms detected | M. tuberculosis, M. leprae, NTM, Nocardia (partial), Cryptosporidium oocysts (modified ZN) |
| Key limitation | Cannot distinguish viable from dead AFB; cannot identify species; cannot detect drug resistance |
| Specimens | Sputum (early morning × 3), BAL, urine, CSF, tissue biopsy, pus |
| Sensitivity threshold | ~5,000–10,000 AFB/mL required for positive smear (vs 10–100 for culture) |
References
- Van Deun, A., Hossain, M. A., Gumusboga, M., & Rieder, H. L. (2008). Ziehl-Neelsen staining: theory and practice. The international journal of tuberculosis and lung disease : the official journal of the International Union against Tuberculosis and Lung Disease, 12(1), 108–110.
- Chen, P., Shi, M., Feng, G. D., Liu, J. Y., Wang, B. J., Shi, X. D., Ma, L., Liu, X. D., Yang, Y. N., Dai, W., Liu, T. T., He, Y., Li, J. G., Hao, X. K., & Zhao, G. (2012). A highly efficient Ziehl-Neelsen stain: identifying de novo intracellular Mycobacterium tuberculosis and improving detection of extracellular M. tuberculosis in cerebrospinal fluid. Journal of clinical microbiology, 50(4), 1166–1170. https://doi.org/10.1128/JCM.05756-11
- Laifangbam, S., Singh, H. L., Singh, N. B., Devi, K. M., & Singh, N. T. (2009). A comparative study of fluorescent microscopy with Ziehl-Neelsen staining and culture for the diagnosis of pulmonary tuberculosis. Kathmandu University medical journal (KUMJ), 7(27), 226–230. https://doi.org/10.3126/kumj.v7i3.2728
- World Health Organization. Tuberculosis Diagnostics Technology and Market Landscape. 5th ed. Geneva: WHO; 2021.
- World Health Organization. Implementing Tuberculosis Diagnostics: A Policy Framework. Geneva: WHO; 2015.
- Steingart KR, Henry M, Ng V, et al. Fluorescence versus conventional sputum smear microscopy for tuberculosis: a systematic review. Lancet Infect Dis. 2006;6(9):570–581. https://doi.org/10.1016/S1473-3099(06)70578-3
Frequently Asked Questions
Why does Ziehl-Neelsen staining require heat while other staining techniques do not?
How is an AFB smear graded and what does the grade mean clinically?
What is the difference between Ziehl-Neelsen and Kinyoun (cold) acid-fast staining?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.