Streptococcus pyogenes (GAS): Properties, Pathogenesis, and Lab Diagnosis
Streptococcus pyogenes (Group A Strep) morphology, virulence factors like M protein and streptolysins, and bacitracin, PYR, and other tests for lab diagnosis.
Popularly known as “flesh-eating bacteria”, Streptococcus pyogenes is one of the pathogenic gram-positive cocci. Streptococcus pyogenes, orGroup A streptococcus (GAS) is mostly known for streptococcal sore throat (strep throat). It is a gram-positive cocci that mostly occurs as chains and occasionally in pairs.
It is the causative agent of acute pharyngitis, impetigo, erysipelas, necrotizing fasciitis (flesh-eating bacteria), and myositis. Other infections caused by this organism are bacteremia with potential infection in any of several organs, pneumonia, scarlet fever, and streptococcal toxic shock syndrome.
Rheumatic fever and acute post-streptococcal glomerulonephritis are two prominent diseases (sequelae) that result due to previous streptococcal infections.
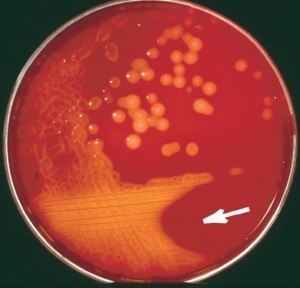 Figure: β-hemolysis by S.pyogenes
Figure: β-hemolysis by S.pyogenes
Image source: Linda Johansson et al. Clin Infect Dis. 2010;51:58-65
Major Characteristics of Streptococcus Pyogenes (GAS)
- Gram-positive cocci
- Non-motile
- Non-sporing
- Fastidious organism; grows well in 5% sheep blood agar (producing β-hemolysis) and chocolate agar.
- Catalase negative (this test helps to differentiate Streptococcus spp from Staphylococcus spp).
- Group A Streptococci: β-Hemolytic streptococci are arranged into groups A-U (Known as Lancefield groups) on the basis of antigenic differences in C carbohydrate.
- Bacitracin sensitive: the growth of S. pyogenes is inhibited by bacitracin, which is an important diagnostic criterion.
Antigen detection methods are used as a screening test. Detection of S. pyogenes antigen in throat specimen is possible by using latex agglutination test, co-agglutination, or ELISA technologies.
Diseases caused by *S.pyogenes*
 Figure: Impetigo
Figure: Impetigo
Streptococcus pyogenes is the leading cause of uncomplicated bacterial pharyngitis and tonsillitis commonly referred to as strep throat. Acute diseases associated with Streptococcus pyogenes occur chiefly in the respiratory tract (sinusitis, otitis), bloodstream (sepsis, endocarditis, meningitis), or the skin (impetigo, cellulitis, necrotizing fasciitis, myositis}.
Noninvasive disease
- Streptococcal sore throat (strep throat)
- Impetigo
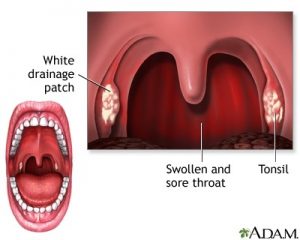 Figure: Streptococcal sore throat (Strep throat) features.
Figure: Streptococcal sore throat (Strep throat) features.
Invasive disease
- Necrotizing fasciitis (NF)
- Streptococcal toxic shock syndrome (STSS)
- Cellulitis
- Bacteremia
- Pneumonia
- Puerperal sepsis
Mnemonic: Diseases caused by Streptococcus pyogenes: NIPPLES: Necrotising fasciitis and myositis, Impetigo, Pharyngitis, Pneumonia, Lymphangitis Erysipelas and cellulitis Scarlet fever/Streptococcal TSS
Nonsuppurative sequelae
- Acute rheumatic fever (ARF)
- Post-streptococcal glomerulonephritis (PSGN)
Two nonsuppurative post-streptococcal sequelae, rheumatic fever, and glomerulonephritis may follow 1-3 weeks after acute illness.
Virulence Factors and How They Cause Disease
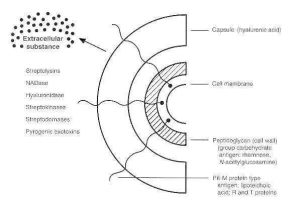 If S. aureus is the burglar who hides in one room and walls itself in with coagulase, S. pyogenes is the arsonist who never stops moving. Nothing here barricades, everything here dissolves and spreads, which is exactly why this organism earned the name "flesh-eating bacteria."
If S. aureus is the burglar who hides in one room and walls itself in with coagulase, S. pyogenes is the arsonist who never stops moving. Nothing here barricades, everything here dissolves and spreads, which is exactly why this organism earned the name "flesh-eating bacteria."
Mnemonic: SMASHED
- Streptolysins (O and S): two separate hemolysins. Streptolysin O is oxygen-labile and strongly immunogenic, which is why ASO antibody titers are useful for retrospective diagnosis. Streptolysin S is oxygen-stable and non-immunogenic, it's actually the one mainly responsible for the visible beta-hemolysis you see on a standard aerobic blood agar plate.
- M protein, the major virulence factor here. It's anti-phagocytic and cytotoxic to neutrophils on its own, but its real significance is structural: it antigenically mimics mammalian cardiac muscle and connective tissue. Clinical link: this molecular mimicry is the direct mechanism behind rheumatic fever, antibodies raised against M protein cross-react with heart tissue weeks after the throat infection has cleared. Lower M-types (1, 3, 5, 6, 14, 18, 19, 24) are the rheumatogenic ones.
- Anti-C5a peptidase: cleaves the complement fragment C5a, which is the chemical signal neutrophils follow to find an infection. Clinical link: this is effectively cutting the alarm wire, neutrophils never get the call to come to the site of infection in the first place.
- Streptokinase: converts plasminogen to plasmin, dissolving fibrin clots. Clinical link: this is the opposite job to coagulase in S. aureus. Where Staph builds a fibrin wall to stay put, Strep dissolves any clot in its way, this is a direct mechanistic reason GAS infections spread diffusely instead of forming a contained abscess.
- Hyaluronidase and hyaluronic acid capsule: hyaluronidase breaks down hyaluronic acid in connective tissue, clearing a path for spread. The capsule itself is chemically identical to host hyaluronic acid, so it's not just physically hiding the organism the way the S. aureus capsule does, it's chemically invisible, the immune system doesn't recognize it as foreign at all.
- Exotoxin (pyrogenic exotoxins SPE A, B, C): superantigens that trigger massive non-specific T-cell activation. SPE A and C are only produced by strains carrying an integrated phage, non-lysogenized strains don't make them. Clinical link: these toxins act directly on the hypothalamus, causing fever, and produce the rash of scarlet fever and the multi-organ involvement of streptococcal toxic shock syndrome.
- DNAses (streptodornase A-D): depolymerize free DNA in pus, thinning it out and helping the infection spread further. DNase B antibody titers, like ASO, are used for retrospective serodiagnosis.
How to Remember the Virulence Factors
Run through SMASHED as a single story instead of seven separate facts: this organism sticks, blinds the alarm system, dissolves everything around it, and leaves a delayed-action trap behind.
The capsule doesn't just hide the bacterium, it's made of the same molecule as your own connective tissue, so your immune system was never going to recognize it as a threat to begin with. Anti-C5a peptidase then cuts the specific signal neutrophils use to find the infection, so even if your body wanted to respond, the call never arrives. Once neutrophils are out of the picture, streptokinase and hyaluronidase go to work dissolving the two things that would normally contain an infection, fibrin clots and connective tissue, which is the direct mechanical reason this organism spreads instead of staying put.
The trap is M protein. It looks so much like your own heart and joint tissue that the antibodies your body eventually makes against it don't stop at the bacterium, weeks later they're still circulating and start attacking your own heart valves. That's rheumatic fever, and it's the single most important fact in this entire section for exam purposes: it's not a separate disease, it's the same M protein story playing out after the infection is already gone.
Key Tests that are used to identify S. pyogenes
The sample for the isolation/identification of S. pyogenes is either pharyngeal exudates, pus, blood, tissue, or body fluids depending on the sites and nature of infection.
Key tests that are commonly employed in diagnostic laboratory for this purpose are:
- Gram Staining (Gram-positive cocci in chains)
- Culture on Blood Agar ( β-Hemolysis)
Grown anaerobically, 100% of strains are beta-hemolytic Grown aerobically, 85% of strains are beta-hemolytic (15% are non-hemolytic)
- Two hemolysins (streptolysins) – O and S
O = encoded by 100% of strains; O2 labile S = encoded by 85% of strains; O2 stable
Biochemical tests
Following biochemical tests are useful for the identification of Streptococcus pyogenes.
| Name of the test | S. pyogenes | |
|---|---|---|
| Catalase test | Negative | Useful to differentiate staphylococci from streptococci |
| Bacitracin sensitivity test | Sensitive | Presumptive identification of group A streptococci (GAS) |
| Pyrrolidonyl-β-naphthylamide (PYR) test | Positive | Presumptive identification of GAS and enterococci |
| CAMP test | Negative | GBS ( S. agalactiae ) is CAMP test positive. |
| Hippurate hydrolysis test | Negative | Streptococcus agalactiae is positive |
Anti-Streptolysin O (ASO) Test: ASO titer is not done for the diagnosis of Streptococcal sore throat but for sequelae (complications) that result due to previous infections with Streptococcus pyogenes.
- Rheumatic fever
- Post streptococcal glomerulonephritis (PSGN)
- Scarlet fever
- Erysipelas
Where students actually get confused
- Bacitracin sensitivity is presumptive, not definitive. Bacitracin-sensitive strongly suggests GAS (and bacitracin-resistant suggests GBS), but a small number of non-group-A strains can also be sensitive. Treat it as a strong screen, confirm with Lancefield grouping or PYR when it matters.
- PYR-positive isn't GAS-specific. Enterococcus is also PYR-positive. A catalase-negative, beta-hemolytic, PYR-positive organism from a throat swab is almost certainly GAS, but PYR alone, out of context, doesn't rule out Enterococcus.
- ASO titer is for sequelae, not acute pharyngitis. Antibodies take 1-3 weeks to develop, so a patient with active strep throat will often have a normal ASO titer. Order it for suspected rheumatic fever or PSGN, not to diagnose the sore throat itself.
- Streptolysin O and S aren't interchangeable in the lab. SLO is what ASO serology detects (it's immunogenic), but SLS is what you're actually looking at when you see beta-hemolysis on a routine aerobic blood plate, since SLO is oxygen-labile and partly inactivated under aerobic conditions.
Key exam facts in one table
| Feature | S. pyogenes | Memory hook |
|---|---|---|
| Gram stain | Cocci in chains | Strep = chains, Staph = clusters |
| Catalase | Negative | Rules out Staph only |
| Hemolysis | Beta | Complete clearing, unlike pneumococcus's partial alpha |
| Bacitracin | Sensitive | GAS is sensitive, GBS is resistant |
| PYR | Positive | Shared with Enterococcus, interpret in context |
| Main spreading enzyme | Streptokinase | The opposite job to S. aureus's coagulase |
| Main immune-evasion factor | M protein | Also the cause of rheumatic fever, same molecule, two jobs |
| Capsule type | Hyaluronic acid, non-antigenic | Chemically invisible, not just hidden |
| Key sequela | Rheumatic fever | M protein mimics heart tissue |
| ASO titer use | Retrospective, for sequelae | Not for diagnosing active sore throat |
Self-check questions
- Why does S. pyogenes cause diffuse, spreading infections while S. aureus tends to form a localized abscess?
- A patient who had a sore throat three weeks ago now has joint pain and a new heart murmur. Which virulence factor explains this, and by what mechanism?
- Why is the S. pyogenes capsule "invisible" to the immune system in a different way than the S. aureus capsule is?
- Why would you order an ASO titer for suspected post-streptococcal glomerulonephritis but not for a patient with active strep throat?
- A throat culture grows catalase-negative, beta-hemolytic, bacitracin-sensitive, PYR-positive cocci in chains. What's the organism, and which single result also fits Enterococcus, meaning it can't be read alone?
References
- Madigan, M. T., Bender, K. S., Buckley, D. H., Sattley, W. M., & Stahl, D. A. (2018). Brock Biology of Microorganisms (15th ed.). Pearson. https://amzn.to/2USOj0v
- Spellerberg, B., & Brandt, C. (2022). Laboratory Diagnosis of Streptococcus pyogenes (group A streptococci). In J. J. Ferretti, D. L. Stevens, & V. A. Fischetti (Eds.), Streptococcus pyogenes: Basic Biology to Clinical Manifestations (2nd ed.). University of Oklahoma Health Sciences Center. https://www.ncbi.nlm.nih.gov/books/NBK587110/
- Hynes, W. (2004). Virulence factors of the group A streptococci and genes that regulate their expression. Frontiers in Bioscience, 9, 3399-3433. https://doi.org/10.2741/1491
Frequently Asked Questions
What is the difference between Streptococcus pyogenes and Streptococcus pneumoniae on a Gram stain?
Can a positive ASO titer diagnose an active strep throat infection?
What is the difference between rheumatic fever and post-streptococcal glomerulonephritis?
Why doesn't S. pyogenes form a walled-off abscess the way S. aureus does?
Why is Streptococcus pyogenes called Group A Streptococcus?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.