Inflammation of hepatocytes (liver cells) is termed hepatitis. The major cause of hepatitis is a viral infection but other causes include excessive consumption of alcohol, toxins, different medications, and autoimmune disorders.
Hepatitis can be classified based on transmissibility into two classes:
- Infectious (viral hepatitis): These include acute Hepatitis caused by hepatitis viruses (A, B, C, D, E, and G) and chronic infection by hepatitis B, hepatitis C, and hepatitis D viruses.
- Non-infectious: Usually, this infection is caused by autoimmune disorders, excessive alcohol consumption, medications, and ingestion of toxins.
Hepatitis A is a fecal-oral transmitted infection often acquired through contaminated food and water. Hepatitis A virus (HAV) causes infectious hepatitis. It is a subacute disease of global distribution, which affects mainly children and young adults.
Table of Contents
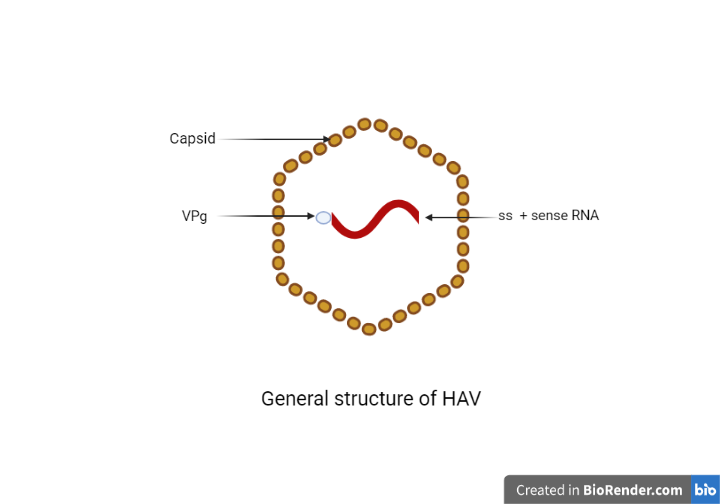
Morphology of Hepatitis A Virus
- HAV is a small (about 27nm) and non-enveloped virus
- It consists of single-stranded positive RNA viruses
- It also consists stable capsid proteins
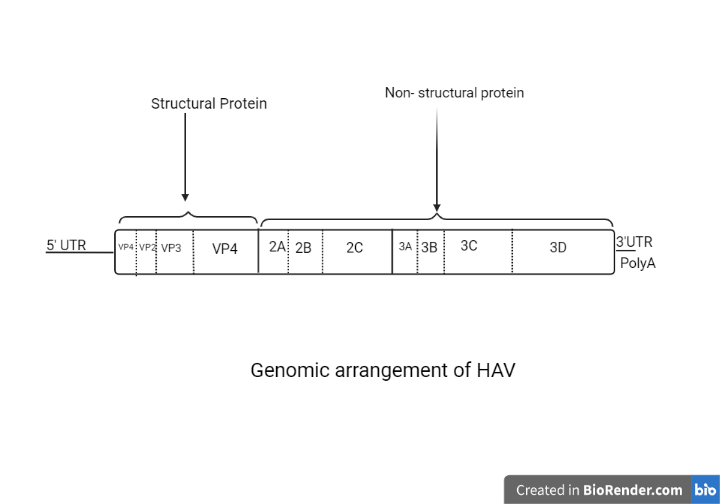
Genomic arrangements
- The genome of hepatitis A virus is single-stranded 7.5kb long with positive polarity (positive sense).
- The organization is similar to other picornaviruses
- Has a very low G+C concentration compared to other picornaviruses.
- The 5’ end is not capped but linked to a viral protein Vpg which is the primer for protein synthesis.
- Most studied genomic strain HM175 suggests that the genome contains only 1 open reading frame flanked by a comparatively long nucleotide sequence of 735 at 5’UTR end and a short 63 nucleotide sequence at 3’UTR end.
- Both UTR segments consisted of the remarkable secondary structure of RNA which was identified with the help of different mapping sites.
- Furthermore, the 3’side of the RNA comprises complex structural elements which play the role of the internal ribosome entry site. (IRES) and helps in cap-independent translation of HAV protein.
Replication of Hepatitis A Virus
Cell entry
- Entry of the virus into cells is from ingestion of the virus. However, the cells that get infected first are a mystery.
- One theory suggests that, although the virus is naked or non-enveloped a pseudo or quasi enveloped (eHAV) enters the liver cells with attachment to the TIM1 (T-Cell immunoglobulin and mucin domain protein 1) a phosphatidyl-serine receptor.
- The receptor is now commonly known as HAVCR1 (HAV cellular receptor 1).
- The binding facilitates the uncoating of the viral genome into the endosomal membranes.
- Even though the role of the receptor-binding mechanism is minor but significant in HAV infection
- Another theory suggests entry via naked virion attaching to the same receptor, this is rapid as a lysosomal step of removing the envelope decreases.
Uncoating of viral material
After the entry, the RNA genome is released inside the cell maybe along with the capsid.
Protein synthesis
- Protein synthesis occurs as soon as the viral genome is released inside the cell.
- Translation of both structural and non-structural proteins is necessary to start RNA replication.
- VPg is removed from the RNA as soon as the release of the RNA. And translation is initiated at a 5’ cap-independent way controlled by IRES.
- Then, the initiation of translation occurs at any one closely attached space of AUG codons resulting in a heterogenous VP4 sequence.
- The IRES is type III which is different from other picornavirus and unlike other enteroviruses, these IRES elements do not shut down host mRNA translation instead both the translation run side by side.
RNA synthesis
- Copying of a positive-strand into a minus strand occurs resulting in the formation of ds-RNA.
- The minus strand is produced from the 3’ end of the genomic RNA primed at uridylated VPg.
- The ds-RNA then helps in the production of new positive-strand genomes.
- The production of positive-strand is similar to negative-strand production but the site is at uridylated VPg at 5’ end.
Virion assembly
The detailed process of assembly of viral particles is less known. But the location of assembly is at the plasma membrane of the host cell.

Pathogenesis
Transmission
- It is highly contagious. The transmission occurs through the fecal-oral route (water and food contaminated with feces of the infected person).
- The reservoir is human beings. Excretion of virus occurs in the first 2 weeks of infection.
- The infected person may be noncontagious after the appearance of jaundice.
Virulence factors
- Survival in extreme environmental conditions
- Resistant to detergents and ethers
Incubation period
The incubation period ranges from15-45 days, but sometimes may stretch to 4 weeks.
- Replication begins from gastrointestinal sites and progresses down to liver cells.
- Although the complete mechanism of destruction of hepatocytes by this virus is unknown. Some speculation suggests the involvement of Cytotoxic T-cells in damaging hepatocytes. It quickly heals after the complete removal of the infection.
- Mononuclear infiltrate, swelling, degeneration, and acidophilic bodies is the result of infection in the hepatocytes which are similar to other viral hepatitis infections.
- Usually, the infection is self-limiting after 2-4 weeks of infection, and once infected the person develops lifelong immunity.
Mortality rate
The mortality rate of HAV infection is <0.01%.
Symptoms
- Tiredness
- Nausea
- Vomiting
- Fever
- Hepatomegaly
- Jaundice
- Anorexia
- Rash
- Passing dark urine, and pale feces.
Laboratory diagnosis of HAV infection
Specimen
- Stool (antigen detection) or serum (antibody detection) of the suspected patient.
Collection and Transport of Stool
Collect the stool in a sterile, leak-proof, and dry container. Preferred amount is 10cc/ml of diarrheal sample. The patient is instructed to collect stool in sterile conditions. As per feasibility and transported to the laboratory within the first 1 hour of collection. If delayed, refrigeration at 4℃ or collection should be done in a container with a viral transport medium.
Collection and Transport of Blood for serum
A serum sample from the same patients is ideal for the correct diagnosis. Blood (15ml from adults and 3ml from children) is drawn aseptically in a tube without anticoagulant. Centrifuge the blood sample in 1000-2000g for 10 minutes. The separated serum sample is then processed. If there is a delay in processing the sample, refrigerate at 4℃ (do not freeze the sample).
(NOTE: if centrifuge is not available, the blood is refrigerated until a clot is formed, the serum is then pipetted into an empty sterile tube and transported to the laboratory as soon as possible.)
Sample processing
Sample process is done by following ways:
Microscopy
An electron microscope can detect viral material in the fecal matter of the suspected individuals.
Virus Isolation
Although virus isolation in human cell lines is possible, it is not applicable during routine diagnosis. But useful for research purposes.
Antigen detection
- Detection of the antigen (viral proteins) of hepatitis A in the stool and sera of the patients 2 weeks before the onset of jaundice to 2 weeks after the onset of jaundice using electron microscopy.
- Similarly, radioimmunoassay and enzyme immunoassay have also helped in the detection of antigens in fecal matters, and cell culture.
Serology
Hepatitis A cannot be distinguished from other types of viral hepatitis on the basis of clinical or epidemiologic features alone. Serology is the primary method for the laboratory diagnosis of hepatitis A virus (HAV) infection.

IgM anti-HAV is the reliable marker of acute infection with hepatitis A virus. Virtually all patients with acute hepatitis A have detectable IgM anti-HAV. Laboratory testing for IgM anti-HAV is typically positive at the time of onset of symptoms (detectable 5/6 days prior to the onset of symptoms). It remains positive for 3-6 months after primary infection. IgG antibodies on the other hand persist for life and indicate immunity against reinfection.
The antibody test for total anti-HAV measures both IgG anti-HAV and IgM anti-HAV. Persons who are total anti-HAV positive and IgM anti-HAV negative i.e. presence of IgG anti-HAV in the absence of IgM anti-HAV indicate past infection or vaccination rather than acute infection.
Molecular Diagnosis
Detection of the nucleic acid of HAV is done in the following ways:
- Restriction fragment length polymorphism (RFLP)
- Southern blotting
- Single-strand conformational polymorphism
- Reverse transcription-PCR
- Antigen capture RT-PCR
Other methods of detection of hepatitis:
- The test for the level of ALT (alanine aminotransferase) and AST (aspartate aminotransferase) in serum is highly useful for the detection of HAV infections as the infections trigger an increase in the level of ALT and AST before the onset of symptoms to 3-10 days after the onset of the symptoms
- Similarly, monitoring serum bilirubin levels is also important. During the appearance of jaundice the level increases. And the decreased level of serum albumin level suggests a serious infection in hepatocytes.
Prevention and Control
No antiviral therapy is necessary only the treatment of symptoms is enough.
Vaccine
Preferably two doses of vaccine at the interval of 6-18 months. There was an anamnestic response when the second dose was taken after several years. Because of this, the timing of the second dose is very crucial.
Prophylaxis with immunoglobulin
Post-exposure immunoglobulin within 2 weeks is recommended in those who are in immediate contact with the infected patients.
The preferred way of administration is a dose of 0.02ml intramuscularly.
Preventing spread
The best way to control the infection is to maintain the cleanliness of drinking water and food by regularly cleaning the water sources, avoiding raw foods, and maintaining personal hygiene.
References:
- Abutaleb, A., & Kottilil, S. (2020). Hepatitis A. Gastroenterology Clinics Of North America, 49(2), 191-199. https://doi.org/10.1016/j.gtc.2020.01.002
- McKnight, K., & Lemon, S. (2018). Hepatitis A Virus Genome Organization and Replication Strategy. Cold Spring Harbor Perspectives In Medicine, 8(12), a033480. https://doi.org/10.1101/cshperspect.a033480
- Nainan, O., Xia, G., Vaughan, G., & Margolis, H. (2006). Diagnosis of Hepatitis A Virus Infection: a Molecular Approach. Clinical Microbiology Reviews, 19(1), 63-79. https://doi.org/10.1128/cmr.19.1.63-79.2006
- Parija, S. (2012). Textbook of Microbiology and Immunology (2nd ed.,) Page 547-550.Elsevier, a division of Reed Elsevier India Private Limited.