Entamoeba histolytica: Life Cycle, Pathogenesis, Liver Abscess, and Laboratory Diagnosis
How does a swallowed cyst cause both bloody dysentery and a liver abscess months later? Complete Entamoeba histolytica life cycle, flask-shaped ulcer mechanism, and lab diagnosis — including how to tell it apart from E. dispar and E. coli.
A 34-year-old man returns from working in an area with poor sanitation, presenting six weeks later with right upper quadrant pain, fever, and a tender, enlarged liver. He has no history of diarrhoea at all. An ultrasound reveals a large abscess in the right lobe of the liver. Aspiration yields thick, brownish-yellow pus with the consistency of anchovy paste.
This presentation is deceptive precisely because it has nothing to do with the intestine on the surface yet it began there. Entamoeba histolytica, ingested as a microscopic cyst in contaminated food or water, can travel silently from the gut to the liver via the portal circulation, causing a destructive abscess in a patient who never had the bloody diarrhoea most people associate with amoebiasis. In fact, in roughly half of liver abscess cases, there is no preceding history of dysentery at all. Understanding the complete journey of this organism — from cyst to trophozoite to tissue invasion to distant organ spread — is what allows a clinician to recognise amoebiasis in its many disguises.
Entamoeba histolytica is an enteric protozoan parasite with worldwide distribution. It is responsible for amoebic dysentery (bloody diarrhea) and invasive extraintestinal amebiasis (such as liver abscess, peritonitis, and pleuropulmonary abscess). Other species of Entamoeba; Entamoeba hartmanii, Entamoeba coli, and Entamoeba dispar do not cause diseases but their trophozoite is difficult to distinguish from those of E.histolytica by light microscopy.
Mode of transmission
Feco-oral route, via the ingestion of contaminated food or water containing mature quadrinucleate cyst of Entamoeba histolytica. Trophozoites if ingested would not survive exposure to the gastric environment.
Mneomonic:EntAmoeba HistoLytica
- Ent: enterocytes (a cell of the intestinal lining);
- Amoeba: protozoa;
- Histo: tissue;
- Lytica: lysis.
Why the Mnemonic Is the Whole Disease in Four Syllables
The mnemonic above is not just a memory device — it is literally the pathophysiology of every clinical manifestation in this article. Histo-lytica (tissue lysis) is the mechanism behind:
- Amoebic dysentery — lysis of colonic mucosa produces the flask-shaped ulcer and the resulting blood and mucus in stool
- Liver abscess — the same cytolytic action, carried by trophozoites to the liver, destroys hepatocytes and produces the anchovy-paste pus described later in this article
- Ameboma — even the granulomatous mass that can mimic colon cancer is a consequence of chronic tissue destruction and the host's reparative response
Every destructive lesion this organism causes, wherever in the body it occurs, traces back to the same enzymatic tissue-lysing capability named directly in its species name. This is worth holding onto as you read the rest of this article — the organism does not have a separate mechanism for the liver and for the gut. It is the same lytic process happening in a different location.
 Figure: Quadrinucleate cyst of Entamoeba histolytica
Figure: Quadrinucleate cyst of Entamoeba histolytica
Infective form: Mature quadrinucleate cyst; it is spherical in shape with a refractile wall
Note:Giardia lamblia cyst also has four nuclei, but the cyst is oval in shape.
Geographical distribution: Worldwide, more common in the tropics and subtropics, especially in areas with poor sanitation (developing and under-developed countries).
Habitat: Trophozoites of E. histolytica live in the mucosal and submucosal layers of the large intestine of man. Life cycle of Entamoeba histolytica has two-stage: motile trophozoite and non-motile cyst. Trophozoites are found in intestinal lesions, extra-intestinal lesions, and diarrheal stools whereas cyst predominates in non-diarrheal stools.
Life cycle of Entamoeba histolytica
Infection by Entamoeba histolytica occurs by the ingestion of mature quadrinucleate cysts in fecally contaminated food, water, or hands. The quadrinucleate cyst is resistant to the gastric environment and passes unaltered through the stomach
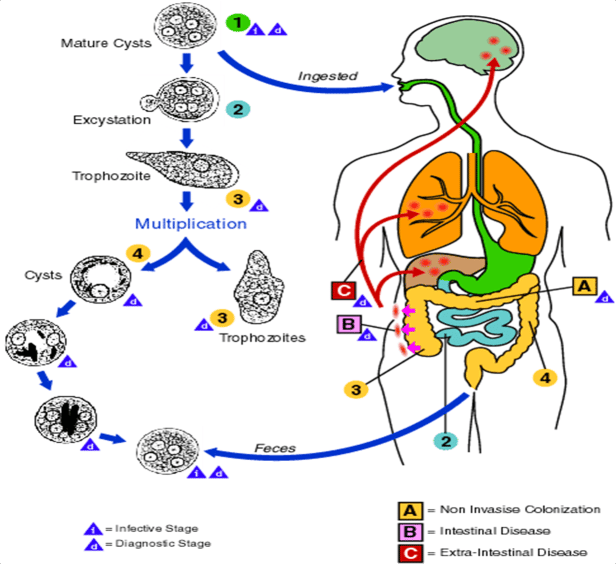 Figure: Life Cycle of Entamoeba histolytica (Source: CDC)
Figure: Life Cycle of Entamoeba histolytica (Source: CDC)
- When the cyst of E.histolytica reaches caecum or lower part of ileum excystation occurs and an amoeba with four nuclei emerges and that divides by binary fission to form eight trophozoites.
- Trophozoites migrate to the large intestine and lodge into the submucosal tissue.
- Trophozoites grow and multiply by binary fission in the large intestine (Trophozoite phase of the life cycle is responsible for producing characteristics lesion of amoebiasis).
- Certain numbers of trophozoites are discharged into the lumen of the bowel and are transformed into cystic forms.
- The cysts thus formed are unable to develop in the same host and therefore necessitate a transference to another susceptible host. The cysts are passed in the feces.
Note: Because of the protection conferred by their walls, the cysts can survive days to weeks in the external environment. Cysts are not highly resistant and are readily killed by boiling. But they are resistant to chlorination or can be removed by filtration. Trophozoites can also be passed in diarrheal stools, but are rapidly destroyed once outside the body.
Trophozoites are responsible for disease conditions;
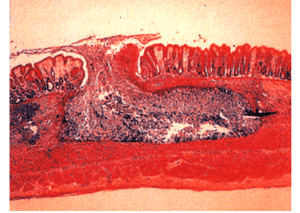 Figure: Flask Shaped Ulcer (Histopathology, UFPA, Araujo R.)
Figure: Flask Shaped Ulcer (Histopathology, UFPA, Araujo R.)
- The trophozoites invade the colonic epithelium and secrete enzymes that cause localized necrosis. Little inflammation occurs at the site.
- As the lesion reaches the muscularis layer, a typical “flask-shaped” ulcer forms, which can undermine and destroy large areas of the intestinal epithelium.
- Progression into submucosa leads to invasion of the portal circulation by the trophozoites.
Diseases
- Non-invasive infection: In many cases, the trophozoites remain confined to the intestinal lumen of individuals who are thus asymptomatic carriers and cysts passers.
- Intestinal disease: In some patients, the trophozoites invade the intestinal mucosa,
- Extra-intestinal disease: through the bloodstream, trophozoites invade extraintestinal sites such as the liver, brain, and lungs, with resultant pathologic manifestations.
Amoebic liver abscess
- About 2-10% of individuals infected with E. histolytica suffer from hepatic complications.
- In 50% of cases, history of amoebic dysentery may not be seen.
- The trophozoites of E.histolytica are carried as emboli by the radicles of the portal vein from the base of amoebic ulcer in the large intestine.
- Capillary system of the liver acts as an efficient filter and holds the trophozoites that multiply inside liver cells and carries on cytolytic actions.
- This leads to obstruction to the circulation and produces thrombosis of the portal venules (sinusoids) resulting in anemic necrosis of the liver cells
- Progressive destruction of concentric layers of liver cells occurs. A large-sized abscess is formed by the coalescence of miliary abscesses.
- Amebic abscess of the liver is characterized by right upper quadrant pain, weight loss, fever, and a tender enlarged liver.
- Right-lobe abscesses can penetrate the diaphragm and cause lung disease (pulmonary amoebiasis)
- Other metastatic lesions: Cerebral amoebiasis, Amoebic pericarditis, Cutaneous amoebiasis, Splenic abscess etc.
- Most cases of amebic liver abscess occur in patients who have not had overt intestinal amebiasis.
- Aspiration of the liver abscess yields brownish-yellow pus with the consistency of anchovy-paste.
Clinical Findings
- Acute intestinal amebiasis dysentery (i.e. bloody, mucus containing diarrhea), lower abdominal discomfort, flatulence.
- Chronic amebiasis: low-grade symptoms such as occasional diarrhea, weight loss, and fatigue also occurs.
- Roughly 90% of infected individuals have an asymptomatic infection but they may be carriers.
- Ameboma, a granulomatous lesion may form in the cecal or rectosigmoid areas of the colon in some patients. These lesions resemble an adenocarcinoma of the colon and must be distinguished from them.
Laboratory diagnosis
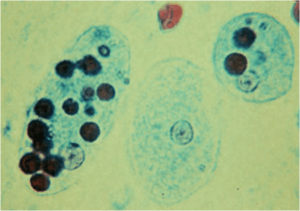 Figure: E.histolytica with ingested RBCs
Figure: E.histolytica with ingested RBCs
Diagnosis of intestinal amebiasis rests on finding either trophozoites in diarrheal stools or cysts in formed stools. Diarrheal stools should be examined within one hour of collection to see the ameboid motility of the trophozoite. The trophozoite characteristically contains ingested red blood cells.
Characteristics of Stool
- Macroscopic appearance of stool: Offensive dark brown semisolid stool, acid in reaction, admixed with blood, mucus, and much fecal matter.
- General microscopic examination: Presence of Charcot-Leyden crystals. Scanty cellular exudates, and consists of only the nuclear masses (pyknotic bodies).E. histolytica infection is distinguished from bacillary dysentery by the lack of high fever and absence PMN leukocytosis.
A. Microscopy
E. histolytica can be distinguished from other amoebas by two major criteria
- Nature of the nucleus of the trophozoite. The E. histolytica nucleus has a small central nucleolus and fine chromatin granules along the border of the nuclear membrane. The nuclei of other amebas are quite different.
Note: The trophozoites of Entamobea dispar, a nonpathogenic species of Entamoeba, are morphologically indistinguishable from those of E. histolytica - Cyst size and the number of its nuclei. Mature cysts of E. histolytica are smaller than those of Entamoeba coli and contain four nuclei, whereas E. coli cysts have eight nuclei.
B. Antigen Detection
Stool antigen detection tests (typically ELISA-based) detect E. histolytica-specific antigens, most notably the Gal/GalNAc lectin. This is a critical advance over microscopy because antigen detection can distinguish E. histolytica from the non-pathogenic E. dispar — something light microscopy cannot do, since their trophozoites and cysts are morphologically identical (see the confusion section below). This makes antigen detection the preferred confirmatory method when microscopy reveals amoebic cysts or trophozoites of uncertain pathogenicity.
C. Serologic Testing
Serology (typically ELISA or indirect haemagglutination, detecting anti-amoebic antibodies) is most useful for invasive disease, particularly amoebic liver abscess, where stool examination is frequently negative (since the trophozoites have left the intestine) and where antigen detection sensitivity is lower than in intestinal disease. Serology is positive in the large majority of liver abscess cases, making it a key diagnostic tool when imaging suggests a hepatic abscess but the cause is not yet confirmed.
Limitation: Antibodies can persist for years after infection clears, so a positive serology in an endemic-area patient does not necessarily indicate current active disease — clinical correlation with imaging and presentation remains essential.
D. Molecular Methods (PCR)
PCR-based assays detect E. histolytica nucleic acid directly from stool, tissue, or aspirate samples, offering high sensitivity and specificity, and — like antigen detection — the ability to distinguish E. histolytica from E. dispar and E. moshkovskii definitively. PCR is increasingly used in reference laboratories and is particularly valuable in research and outbreak settings, though it remains less widely available than microscopy or antigen testing in resource-limited settings.
Treatment
Treatment depends on whether the infection is luminal (asymptomatic cyst passage) or invasive (intestinal or extra-intestinal disease) — this distinction matters because the two drug classes used have different targets:
| Disease state | Treatment | Why |
|---|---|---|
| Asymptomatic cyst passer (luminal infection only) | Luminal agent — e.g., diloxanide furoate or paromomycin | Clears intestinal colonisation; tissue-acting drugs are not needed since there is no invasion |
| Invasive intestinal disease (amoebic dysentery) | Tissue-acting agent (metronidazole or tinidazole) followed by a luminal agent | Metronidazole treats active tissue invasion; the luminal agent afterward eliminates any remaining intraluminal cysts/trophozoites to prevent relapse and continued transmission |
| Amoebic liver abscess | Tissue-acting agent (metronidazole or tinidazole) followed by a luminal agent | Same two-drug logic — metronidazole resolves the abscess; the luminal agent clears the intestinal reservoir that seeded it |
Why the two-drug sequence matters clinically: Metronidazole alone treats invasive tissue disease effectively but has poor activity against organisms remaining in the bowel lumen. Treating only with metronidazole and stopping once symptoms resolve can leave intraluminal cysts behind — leading to relapse and, just as importantly from a public health perspective, continued transmission to others through cyst shedding. This is the most commonly tested treatment principle for this organism.
Most amoebic liver abscesses respond to medical therapy alone; percutaneous or surgical drainage is reserved for large abscesses, abscesses at risk of rupture, or those not responding to medical treatment.
Where Students Actually Get Confused
1. "If the trophozoite looks like E. histolytica under the microscope, it is E. histolytica." Not necessarily. Entamoeba dispar — a genetically distinct, non-pathogenic species — has trophozoites and cysts that are morphologically indistinguishable from E. histolytica by light microscopy, as the article already notes. E. dispar is in fact more common than E. histolytica in many populations. This is precisely why antigen detection or PCR is required to confirm pathogenic infection when treatment decisions depend on it — morphology alone cannot make this call.
2. "More nuclei in a cyst always means it's a different, more dangerous species." The opposite logic applies here. E. histolytica mature cysts have four nuclei and are smaller; Entamoeba coli (a non-pathogenic commensal) cysts have up to eight nuclei and are larger. More nuclei, in this specific comparison, points to the harmless species, not a more dangerous one.
3. "A four-nucleated cyst in stool is always Entamoeba histolytica." As the article notes, Giardia lamblia cysts also contain four nuclei — but Giardia cysts are oval, while E. histolytica cysts are spherical. Nuclei count alone is not sufficient; shape must be considered together with nuclei count, especially when differentiating from Giardia.
4. "A patient with a liver abscess must have had bloody diarrhoea first." As the article states explicitly, roughly half of amoebic liver abscess cases have no preceding history of dysentery. The absence of a diarrhoeal history should not lower clinical suspicion for amoebic liver abscess in the right epidemiological context (travel history, endemic area, compatible presentation).
5. "Ameboma is a tumour." An ameboma is a granulomatous inflammatory mass, not a neoplasm — but as the article correctly notes, it can closely resemble colonic adenocarcinoma both clinically and on imaging, particularly in the caecal or rectosigmoid regions. Distinguishing the two is clinically important precisely because the appropriate management is entirely different (antiamoebic therapy vs oncological workup and treatment), and misdiagnosis in either direction carries real consequences.
6. "Amoebic dysentery and bacillary dysentery present identically." The article already provides the key distinguishing features: amoebic dysentery characteristically lacks the high fever and peripheral PMN leukocytosis seen in bacillary (e.g., Shigella) dysentery. This is a frequently tested bedside distinction, since both can present with bloody, mucoid stool.
7. "Treating with metronidazole alone is sufficient for invasive amoebiasis." Metronidazole is highly effective against invasive tissue disease but has limited activity against organisms remaining in the intestinal lumen. Without a follow-up luminal agent, residual intraluminal infection can cause relapse and ongoing transmission via cyst shedding — this is a key, commonly tested treatment principle (see Treatment section above).
Key Exam Facts in One Table
| Fact | Detail | Memory hook |
|---|---|---|
| Mnemonic | Ent (enterocytes) + Amoeba + Histo (tissue) + Lytica (lysis) | The name IS the pathophysiology |
| Infective form | Mature quadrinucleate cyst | Spherical, refractile wall |
| Cyst vs Giardia cyst | Both 4 nuclei — but E. histolytica is spherical, Giardia is oval | Shape distinguishes them |
| E. histolytica vs E. coli cyst | Histolytica: 4 nuclei, smaller; E. coli: up to 8 nuclei, larger | More nuclei = harmless commensal here |
| E. histolytica vs E. dispar | Morphologically IDENTICAL trophozoites/cysts | Antigen detection or PCR required to differentiate |
| Trophozoite habitat | Mucosal/submucosal layers of large intestine | Cysts in formed stool; trophozoites in diarrhoeal stool |
| Diagnostic hallmark on smear | Trophozoite with ingested RBCs | Confirms active tissue invasion |
| Classic lesion | Flask-shaped ulcer | Narrow neck, wide base in submucosa |
| % asymptomatic carriers | ~90% | Most infections are silent |
| % with hepatic complications | 2–10% | Liver abscess is the major extraintestinal disease |
| % liver abscess with no prior dysentery history | ~50% | Absence of diarrhoea history doesn't exclude it |
| Classic liver abscess pus | Brownish-yellow, "anchovy paste" consistency | Distinctive aspirate description |
| Amoebic vs bacillary dysentery | Amoebic: no high fever, no PMN leukocytosis | Key bedside distinguishing feature |
| Stool microscopy finding | Charcot-Leyden crystals; scanty exudate (pyknotic bodies) | Different pattern from bacterial dysentery |
| Luminal-only treatment | Diloxanide furoate or paromomycin | For asymptomatic cyst passers |
| Invasive disease treatment | Metronidazole/tinidazole + luminal agent afterward | Two-drug sequence prevents relapse/transmission |
| Ameboma mimics | Colonic adenocarcinoma | Granulomatous mass, not a tumour |
Self-Check Questions
- A stool microscopy report describes a trophozoite morphologically consistent with E. histolytica, but the laboratory cannot determine whether it is pathogenic. What test should be ordered next, and why can't morphology alone answer this question?
- A patient presents with a liver abscess but denies ever having diarrhoea. Does this rule out amoebic liver abscess as the cause?
- Why does treatment of invasive amoebic disease require both a tissue-acting agent and a luminal agent, rather than metronidazole alone?
- A stool sample shows a spherical cyst with four nuclei. A colleague suggests this could be either Entamoeba histolytica or Giardia lamblia. How would you distinguish between the two possibilities using this description alone?
- Explain, using the species name itself, why Entamoeba histolytica is capable of causing disease in both the intestine and the liver through the same basic mechanism.
- A colonic mass on imaging is suspected to be either an ameboma or adenocarcinoma. Why does this distinction matter clinically, even though both can look similar?
Answers
- Antigen detection (ELISA for Gal/GalNAc lectin) or PCR should be ordered. Morphology alone cannot distinguish pathogenic E. histolytica from the non-pathogenic E. dispar, since their trophozoites and cysts are identical under light microscopy. Only antigen-based or molecular methods can confirm which species is actually present, which is essential before deciding on treatment.
- No. Approximately 50% of amoebic liver abscess cases occur without a preceding history of overt intestinal amoebiasis or dysentery. The absence of a diarrhoeal history should not lower clinical suspicion in a patient with a compatible presentation and relevant epidemiological risk factors.
- Metronidazole (or tinidazole) is highly effective against invasive tissue disease but has limited activity against organisms remaining in the intestinal lumen. Without a follow-up luminal agent (such as diloxanide furoate), residual cysts or trophozoites in the bowel can cause relapse of disease and continued transmission to others through cyst shedding in stool.
- Shape is the key distinguishing feature given identical nuclei count. A spherical four-nucleated cyst is consistent with Entamoeba histolytica; an oval four-nucleated cyst is consistent with Giardia lamblia. Nuclei count alone (both organisms can show four nuclei) is insufficient — the overall shape of the cyst must also be assessed.
- The species name itself encodes the mechanism: "Histo" (tissue) + "Lytica" (lysis) describes a tissue-lysing enzymatic capability that is not site-specific. The same cytolytic action that destroys colonic mucosa to form the flask-shaped ulcer in the intestine is carried by trophozoites via the portal circulation to the liver, where it destroys hepatocytes to form an abscess. It is one underlying mechanism producing different lesions depending on where the trophozoites end up.
- The two conditions require entirely different management — an ameboma is treated with antiamoebic therapy, while adenocarcinoma requires oncological workup and treatment (which may include surgery, chemotherapy, or radiotherapy). Misdiagnosing one as the other in either direction risks either unnecessary oncological intervention or a missed cancer diagnosis, making accurate differentiation clinically essential despite the lesions' similar appearance.
References and further readings
- Sastry, A. S., & Bhat, S. (2014). Essentials of Medical Parasitology. Jaypee Brothers Medical Publishers (P) Ltd.
- Garcia, L. S. (2016). Diagnostic Medical Parasitology (6th ed.). ASM Press.
- Shirley, D. T., Farr, L., Watanabe, K., & Moonah, S. (2018). A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infectious Diseases, 5(7), ofy161. https://doi.org/10.1093/ofid/ofy161
- Stanley, S. L. Jr. (2003). Amoebiasis. The Lancet, 361(9362), 1025–1034. https://doi.org/10.1016/S0140-6736(03)12830-9
- Haque, R., Huston, C. D., Hughes, M., Houpt, E., & Petri, W. A. Jr. (2003). Amebiasis. New England Journal of Medicine, 348(16), 1565–1573. https://doi.org/10.1056/NEJMra022710
- World Health Organization. (1997). Amoebiasis. Weekly Epidemiological Record, 72(14), 97–99.
Frequently Asked Questions
How does Entamoeba histolytica cause both intestinal disease and liver abscess?
How is Entamoeba histolytica distinguished from Entamoeba dispar?
Why is the treatment of invasive amoebiasis a two-drug sequence rather than metronidazole alone?
Can a patient have an amoebic liver abscess without ever having had diarrhoea?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.