E-Test (Epsilometer): Why It Beats a Plain Disc Test, Procedure & Reading Rules
E-test gives an exact MIC value, not just a Susceptible/Resistant call. Full procedure, strip placement, and the reading rules that trip up most students — plus how E-test strips are used to screen for ESBL.
Epsilometer test (E- test ) is an ‘exponential gradient’ method of determination of antimicrobial resistance. The E-test has been developed to provide a direct quantification of antimicrobial susceptibility of microorganisms. This is a quantitative method that applies both the dilution of antibiotics and diffusion of antibiotics into the medium.
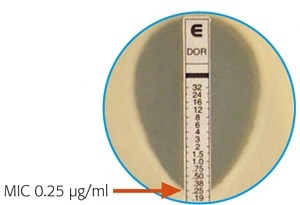 Figure: E-Test showing MIC
Figure: E-Test showing MIC
The device consists of a predefined, continuous, and exponential gradient of antibiotic concentrations immobilized along a rectangular plastic test strip. After 18–24 hours of incubation (longer for slow-growing organisms), a drop-shaped inhibition zone intersects the graded test strip at the inhibitory concentration (IC) of the antibiotic.
Why Use E-Test Instead of a Plain Disc Test?
Standard disc diffusion gives a category — Susceptible, Intermediate, or Resistant — and that's enough for most infections. E-test exists for the cases where a category isn't precise enough and you need the actual number.
Borderline calls matter most where the margin for error is smallest. A vancomycin MIC of 2 μg/mL versus 0.5 μg/mL can both fall in the "Susceptible" range by disc diffusion, yet the higher end of that range is associated with worse outcomes in MRSA bacteremia — a difference a categorical S/I/R report alone won't show you. This is exactly why E-test gets reached for in serious, borderline, or treatment-failure cases rather than run on every isolate by default — it's quantitative precision where it actually changes a decision, not a routine replacement for disc diffusion.
E-test strips are also used in a way disc diffusion can't replicate: dual-ended combination strips carry an antibiotic alone on one end and the same antibiotic plus a β-lactamase inhibitor (like clavulanic acid) on the other. Comparing the two MICs on a single strip is a direct, quantitative way to screen for ESBL production — see the Beta-Lactamase Classification article for what a positive result implies clinically.
HOW IT WORKS?
- A predefined stable antimicrobial gradient is present on a thin inert non-porous plastic carrier strip 5mm wide, 60 mm long known as E-test strip.
- When this E test strip is applied onto an inoculated agar plate, there is an immediate release of the drug and the establishment of an antimicrobial concentration gradient in an agar medium.
- After overnight incubation, the tests are read by viewing the strips from the top of the plate, a symmetrical inhibition ellipse is produced.
- The intersection of the lower part of the ellipse-shaped growth inhibition area with the test strip indicates the MIC value.
REQUIREMENTS
MEDIA: Mueller Hinton agar (MHA) plates (uniform depth of 4 mm)
OTHERS
- E-test strips (of desired antibiotic)
- McFarland standard 0.5
- Forceps
- Sterile cotton swabs
- Sterile normal saline, 4 ml volumes in tubes
Bacterial strains• Non-fastidious cultures plated out for single colonies.• Strain for quality control: Escherichia coli ATCC 25922
PROCEDURES
- Inoculum Preparation
- Remove the E-test package from the freezer (-20°C) at least 30 minutes before required.
- Emulsify 3 or 4 individual test strain colonies and transfer to a tube of saline.
- Compare turbidity to that in the 0.5 McFarland standards. Adjust turbidity of inoculum to match that standard.
- Inoculation in Muller Hinton Agar
- Dip a sterile cotton swab into the inoculums and pulling out slightly, rotate the swab several times against the inside of the tube above the fluid level to remove excess liquid.
- Streak the swab over the entire surface of the agar plate by rotating the plate approximately 60o. Complete inoculation by running the swab around the rim of the agar.
- Leave the lid of the plate ajar for 5 minutes (no more than 15 minutes) to allow any excess moisture to be absorbed before applying strips.
NOTE: Swab plate within 15 minutes of preparing the adjusted inoculums
- Application of E-test strips:
- Open E-test package by cutting package along the broken line. Apply strips to agar surface using forceps (or E-test applicator if available).
- Place the strip with the ‘E end’ at the edge of the plate and with the scale visible (i.e. facing upwards).
- If strips stick together, they may be pulled apart by handling the section marked E. Do not touch any other area of the strip.
- Use templates to position 4 to 6 strips onto a 150 mm plate or one (seldom two) strips onto a 90 mm plate. Do not remove or replace a strip once it has touched the agar.
- Repeat the entire procedure also for Quality control Strain (E. coli ATCC 25922)
- Incubate Plates at 37°C for 18-24 hrs.
Result and Interpretation
 Figure: A Staphylococcus aureus isolate tested by the E-test gradient diffusion method
Figure: A Staphylococcus aureus isolate tested by the E-test gradient diffusion method
- Read MIC at the point where the ellipse intersects the scale. If the value falls between two twofold dilutions, always round up to the next highest value — this keeps readings consistent with the twofold steps used in broth/agar dilution, so MICs from different methods stay comparable.
- Read at complete inhibition of all growth. Faint haze or isolated colonies within the ellipse are not counted as growth for this purpose.
- If the intersection differs on either side of the strip, read the greater value, and ignore any growth right at the strip's edge. This is a deliberately conservative rule: a plate is never perfectly uniform, and erring toward the higher MIC avoids under-calling resistance from whichever side of the ellipse happened to grow back less.
MIC values of the bacteria should be interpreted as S (Susceptible), I (Intermediate), or R (Resistant) by comparing the breakpoint values of each antibiotic with the criteria recommended by CLSI.
E-Test vs. Disc Diffusion vs. Broth/Agar Dilution
| Disc Diffusion (Kirby-Bauer) | E-Test | Broth/Agar Dilution | |
|---|---|---|---|
| Result type | Qualitative — S/I/R only | Quantitative MIC + S/I/R | Quantitative MIC + S/I/R |
| Relative cost | Low | Higher (commercial strips) | Low reagent cost, labor-intensive |
| Throughput | High — many drugs per plate | Lower — 4–6 strips per large plate | Low — batch setup required |
| Typical role | Routine, first-line screening | Confirming borderline or critical MICs; ESBL screening with combination strips | Reference method; required for fastidious organisms and some drug classes |
| Turnaround | 16–24h | 18–24h (longer for slow growers) | 16–24h |
Learning & Remembering
Clinical story: Why E-Test Instead of a Plain Disc Test (above) — the borderline vancomycin MIC, and the dual-ended ESBL screening strip.
One sentence that captures it: Disc diffusion tells you yes or no; E-test tells you by how much — and "by how much" is exactly what matters when the margin between working and failing is thin.
Exam facts
| Question | Answer |
|---|---|
| E-test strip dimensions? | 5 mm wide, 60 mm long |
| Type of antibiotic gradient on the strip? | Continuous, exponential |
| Media used? | Mueller-Hinton agar, 4 mm uniform depth |
| Standard incubation? | 37°C, 18–24 hours (longer for slow-growing organisms) |
| QC strain? | E. coli ATCC 25922 |
| If the MIC falls between two twofold dilutions, which way do you round? | Up |
| If the ellipse intersects at different points on either side of the strip? | Read the greater (higher) value |
| How does E-test detect ESBL production? | Dual-ended strip — antibiotic alone vs. antibiotic + β-lactamase inhibitor; a large MIC drop with the inhibitor present is positive |
References
- Nachnani, S., Scuteri, A., Newman, M. G., Avanessian, A. B., & Lomeli, S. L. (1992). E-test: a new technique for antimicrobial susceptibility testing for periodontal microorganisms. Journal of Periodontology, 63(7), 576–583. https://doi.org/10.1902/jop.1992.63.7.576
- Brown, D. F., & Brown, L. (1991). Evaluation of the E test, a novel method of quantifying antimicrobial activity. The Journal of Antimicrobial Chemotherapy, 27(2), 185–190. https://doi.org/10.1093/jac/27.2.185
- CLSI. M100—Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute; current annual edition.
Frequently Asked Questions
What's the difference between E-test and disc diffusion?
Why does E-test use an exponential antibiotic gradient instead of a fixed concentration?
If the inhibition ellipse intersects at different points on either side of the strip, which value do you read?
How is E-test used to screen for ESBL production?
Why is Mueller-Hinton agar used for E-test, and why does the depth matter?
Is E-test used routinely on every isolate?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.