Bacitracin Test: Principle, Procedure, Results
Bacitracin susceptibility test principle, procedure, and zone interpretation for presumptive identification of Streptococcus pyogenes (Group A Strep)
Bacitracin is a bactericidal drug that is useful in treating superficial skin infections but is too toxic for systemic use. Bacitracin is a polypeptide antibiotic produced by Bacillus subtilis.
Bacitracin interferes with the peptidoglycan synthesis of bacteria. The presumptive identification of group A streptococci (GAS) is usually made by testing for sensitivity to bacitracin.
Principle
Bacitracin test is used to determine the effect of a small amount of bacitracin (0.04 IU or 0.05 IU not higher) on an organism. Streptococcus pyogenes (Group A Streptococci) is inhibited by the small amount of bacitracin in the disk; other beta-hemolytic streptococci usually are not. Some laboratories do not recommend the use of 0.04 U bacitracin disk as Lancefield groups C and G streptococci may occasionally also show susceptibility to bacitracin. PYR reaction can confirm the isolate as S. pyogenes as it’s the only beta-hemolytic streptococci that gives a positive PYR reaction.
 Figure: Identification chart for Gram-positive cocci Source: sigmaaldrich.com
Figure: Identification chart for Gram-positive cocci Source: sigmaaldrich.com
Bacitracin is one of three disk-diffusion tests used to separate look-alike Gram-positive cocci, alongside optochin (for S. pneumoniae among the alpha-hemolytic streptococci) and novobiocin (for S. saprophyticus among the coagulase-negative staphylococci). Which one you reach for depends on the catalase and hemolysis results you already have. See the Gram-positive coccus disk-test grid on the optochin sensitivity test article for the full routing.
Quality Control
Perform sterility and performance testing blood agar plate and/or chocolate agar plate according to CLSI guidelines. Test the disk potency after each shipment or purchase of the bacitracin disk with the appropriate test organism.
| Test organism | Bacitracin (0.04 IU) result |
|---|---|
| Streptococcus pyogenes ATCC 19615 | Zone of inhibition (sensitive) |
| Streptococcus agalactiae ATCC 13813 | No zone (resistant) |
Test each new lot of 0.04 IU differential disks with a known Group A (sensitive) and a known non-Group A beta-hemolytic (resistant) control.
Procedure of Bacitracin test
- Using an inoculating loop, streak two or three suspect colonies of a pure culture onto a blood agar plate.
- Using heated forceps, place a bacitracin disk in the first quadrant (area of heaviest growth). Gently tap the disk to ensure adequate contact with the agar surface.
- Incubate the plate for 18 to 24 hours at 35°C in CO2.
- Look for a zone of inhibition around the disk.
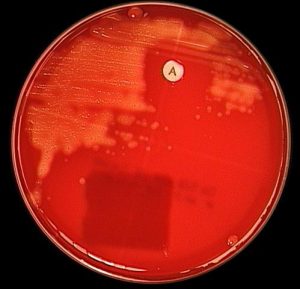 Figure: Bacitracin (A disk) test for identifying Streptococcus pyogenes.
Figure: Bacitracin (A disk) test for identifying Streptococcus pyogenes.
Note: If used on direct sputum culture plates, use chocolate agar for bacitracin and blood agar plate for optochin. Addition of bacitracin disk (not Taxo A) to chocolate agar inhibits upper respiratory microbiota and improves detection of Haemophilus influenzae.
Results
- Bacitracin sensitive: Any zone of inhibition around the disk. For example, Streptococcus pyogenes
- Bacitracin resistant: No zone of inhibition around the disk. Streptococcus agalactiae
A second use: separating Staphylococcus from Micrococcus
Besides identifying Group A strep, the Taxo A bacitracin disk separates two catalase-positive Gram-positive cocci that are easy to confuse: Staphylococcus (resistant) and Micrococcus (susceptible). All staphylococci, including coagulase-negative species, are resistant and show no zone; micrococci are inhibited and show a zone. This is the reverse logic from the strep test in one sense: here a zone points away from Staphylococcus, toward Micrococcus.
This is why bacitracin appears twice in the Gram-positive coccus workup, once on the catalase-negative side (Group A strep among the beta-hemolytic streptococci) and once on the catalase-positive side (Micrococcus vs Staphylococcus). The catalase result tells you which question you are asking. For the staph-vs-micrococcus use, the modification test and lysostaphin are alternative confirmations.
Where students actually get confused
- Reading bacitracin straight off a primary culture plate is less reliable than from a pure subculture. Mixed flora and overcrowded colonies near the disk are the main causes of misreads on primary plates. If a primary-plate result looks ambiguous, a purified subculture, not a second look at the same plate, is the right next step.
- Any zone counts as sensitive, there's no minimum size cutoff. This is different from the optochin test, where zone size matters (≥14mm vs the 9-13mm equivocal range). Bacitracin is a binary call: any visible zone of inhibition, however small, is sensitive. No zone at all is resistant. Don't import optochin's measurement logic here.
- Sensitivity isn't 100% specific to GAS. Group C and G streptococci occasionally show susceptibility too. When that matters, a PYR test resolves it, S. pyogenes is the only beta-hemolytic strep that's PYR-positive.
- Chocolate agar vs blood agar matters in combined respiratory cultures. When bacitracin and optochin are both used on a single throat or sputum workup, bacitracin goes on chocolate agar (it suppresses normal upper respiratory flora and improves H. influenzae detection), while optochin goes on blood agar. Mixing these up affects both readings.
- 0.04 IU is a screening concentration, not a treatment dose. Don't conflate this lab test concentration with bacitracin's therapeutic use, they're testing two different things (presumptive identification vs. treating an infection).
Key exam facts in one table
| Feature | Detail | Memory hook |
|---|---|---|
| Identifies | Streptococcus pyogenes (GAS), presumptively | |
| Disk potency | 0.04-0.05 IU | Low concentration, screening only |
| Mechanism | Interferes with peptidoglycan synthesis | |
| Result rule | Any zone = sensitive, no zone = resistant | No size cutoff, unlike optochin |
| GAS result | Sensitive | Opposite of GBS |
| Occasional false positives | Group C, G streptococci | Confirm with PYR |
| Combined culture media | Chocolate agar (not blood agar) | When paired with optochin workup |
How to Remember
This is the same flip you already know from the GAS/GBS comparison: GAS is bacitracin-sensitive, GBS is resistant. If you've internalized that contrast, this test isn't new information, it's just the bench version of a fact you already have.
A useful bit of irony to anchor it: bacitracin itself is a topical antibiotic used for minor skin infections, too toxic for systemic use. The organism this test identifies, S. pyogenes, is also one of the most common causes of the kind of superficial skin and throat infections bacitracin ointment treats. The drug and the diagnostic test share the same organism on opposite ends, one treats it, one identifies it.
References
- Murray, P. R., Wold, A. D., Hall, M. M., & Washington, J. A., 2nd (1976). Bacitracin differentiation for presumptive identification of group A beta-hemolytic streptococci: comparison of primary and purified plate testing. The Journal of pediatrics, 89(4), 576–579. https://doi.org/10.1016/s0022-3476(76)80389-7
- Katz, B. E., & Fisher, A. A. (1987). Bacitracin: a unique topical antibiotic sensitizer. Journal of the American Academy of Dermatology, 17(6), 1016–1024. https://doi.org/10.1016/s0190-9622(87)70292-8
- Procop GW, Church DL, Hall GS, Janda WM, Koneman EW, Schreckenberger PC, Woods GL. Koneman's Color Atlas and Textbook of Diagnostic Microbiology. 7th ed. Philadelphia: Wolters Kluwer; 2017.
- Tille PM. Bailey and Scott's Diagnostic Microbiology. 15th ed. St. Louis: Elsevier; 2022.
- Jelinková J, Rotta J. The bacitracin test for the recognition of group A streptococci. Int J Syst Bacteriol. 1967;17(3):297.
- Ben-Zaken H, et al. Differentiation of Staphylococcus and Micrococcus spp. with the Taxo A bacitracin disk. J Clin Microbiol.
Frequently Asked Questions
Does the bacitracin test need a minimum zone size to count as sensitive?
Can organisms other than Streptococcus pyogenes be bacitracin sensitive?
Why does it matter which agar the bacitracin disk is placed on in a throat culture?
How does the bacitracin test identify Group A streptococci?
Why is the PYR test used alongside bacitracin?
Why is there no zone-size cutoff in the bacitracin test?
Why should bacitracin be read from a pure subculture rather than a primary plate?

Tankeshwar Acharya, MSc (Medical Microbiology)
Tankeshwar Acharya is an Assistant Professor in the Department of Microbiology at Patan Academy of Health Sciences (PAHS), Nepal, where he has been teaching and practicing clinical microbiology for over 14 years. He is the founder of Microbe Online, one of the leading free microbiology education resources on the web, covering bacteriology, mycology, parasitology, immunology, and clinical laboratory diagnostics written from direct experience in both the classroom and the diagnostic laboratory.